PREVENTIVE TREATMENT MIGRAINE, TENSIONAL AND CLUSTER HEADCHE
Jessica García Alhama
Joan Prat Rojo
Mariano Huerta Villanueva
Unidad de Cefaleas. Servicio de Neurología.
Hospital de Bellvitge. Hospital de Viladecans.
We know about symptomatic treatments of migraine, tensional and cluster headache but preventive treatment guidelines are sometimes ambiguos about treatment recommendation. We review preventive treatment for each headache.
MIGRAINE
Migraine is an episodic headache that typically occurs with a duration of 4 to 72 hours, usually unilateral and throbbing character location, moderate or severe intensity, which worsens with physical activity and is associated with nausea or photophobia and phonophobia. It may be accompanied or preceded by episodes of neurological, transient focal, which develop gradually and is known as aura. In the case of presenting headache for 15 days or more per month for more than three months and at least 8 days per month correspond to migraine headache we are talking about chronic migraine.
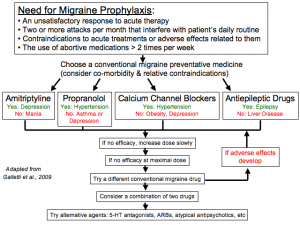
It is recommended to start preventive treatment in patients who have at least three migraine attacks per month, or severe intensity crisis, or poor response or contraindications to symptomatic treatment or if they have prolonged or incapacitating crisis with aura. It is important to assess the existence of triggers for the crisis to try to avoid as far as possible.
We recommend keeping preventive treatment alone, between 3 and 6 months, gradually withdrawing, and consider that its effect starts after 2-4 weeks. To say that a treatment is not effective must spend two months in treatment and optimal dose.
The following table treatments more evidence for the preventive treatment of migraine are discussed.
TENSIONAL HEADACHE
Tensional headache is typically holocraneal in location but can dominate an area. Usually oppressive, mild or moderate in intensity, it can last from minutes to days, and does not worsen with routine physical activity is associated with vomiting or even may be accompanied by nausea. It may be associated with photophobia or phonophobia. It can occur episodically infrequent or frequent, or evolve into a chronic form with daily pain and affect everyday life.
It is advisable to ask a preventive treatment and reduce the use of NSAIDs for analgesia or minimize the risk of developing medication overuse headache. The drugs most used as a preventive treatment in this type of headache include tricyclic antidepressants like amitriptyline, with a level of evidence A, and if not tolerated or no answer is obtained, can be used mirtazapine, level of evidence B.
In addition to receiving adequate pharmacological treatment, these patients should try to change all the factors that have led to the development of chronic pain. Chronic tensional headaches may require psychiatric assessment or referral to psychology.
Then drugs more effectively and more used for preventive treatment of tensional headache are exposed.

CLUSTER HEADACHE
The cluster headache or cluster, is characterized as a unilateral pain, peri or supraorbital or temporal, between 15 and 180 minutes, which is accompanied by ipsilateral autonomic disorders such as conjunctival injection, lacrimation, nasal congestion, runny nose, eyelid edema, Front sweating, ptosis or miosis, plus restlessness and agitation. It has a frequency of between 1 episode every two days to several a day, with a predominance in the afternoon and evening.
It can present with an episodic pattern with symptomatic periods of weeks or months and asymptomatic periods longer than a month or years, and a chronic pattern in which there are no free periods longer than one month over a year crisis.
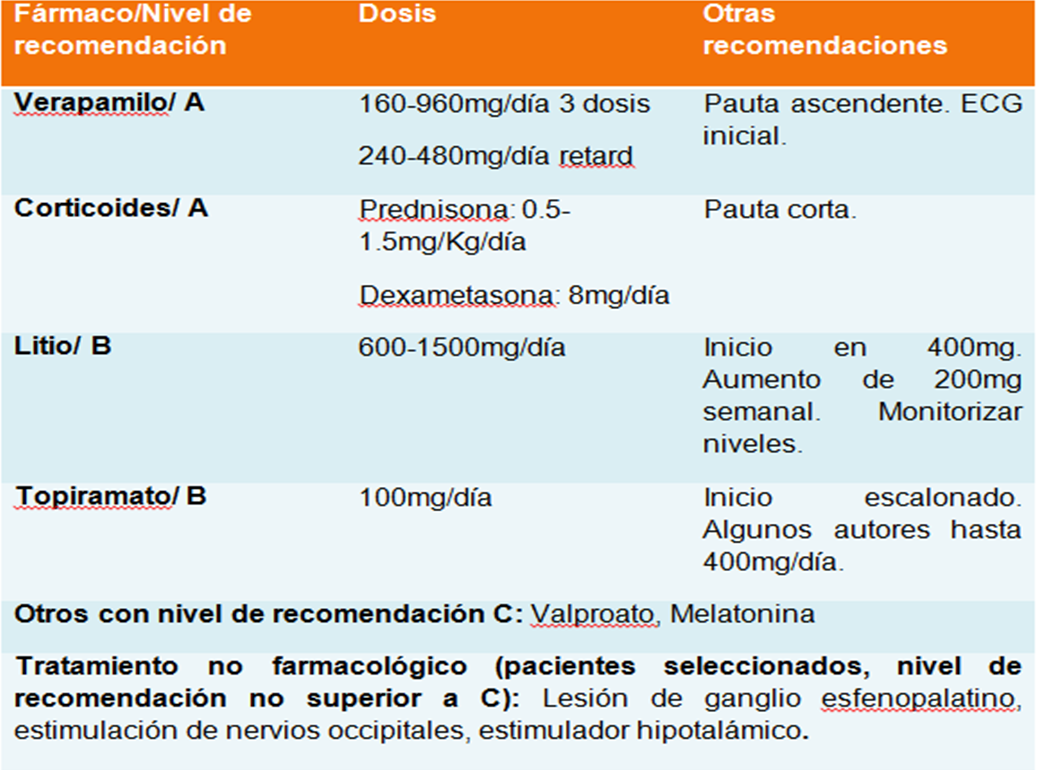
At the start of a symptomatic period, we recommend corticosteroids associated with verapamil, given the rapid action of steroids and verapamil takes about two weeks to start its effect. Verapamil is maintained until a few weeks after completion of the symptoms.
Table: preventive treatments for cluster headache according to the recommended order are shown below.