Certainly as much other cardiovascular ischemic disease the lower the TA after a stroke he is associated with decreased cardiovascular risk, although always with certain precautions.
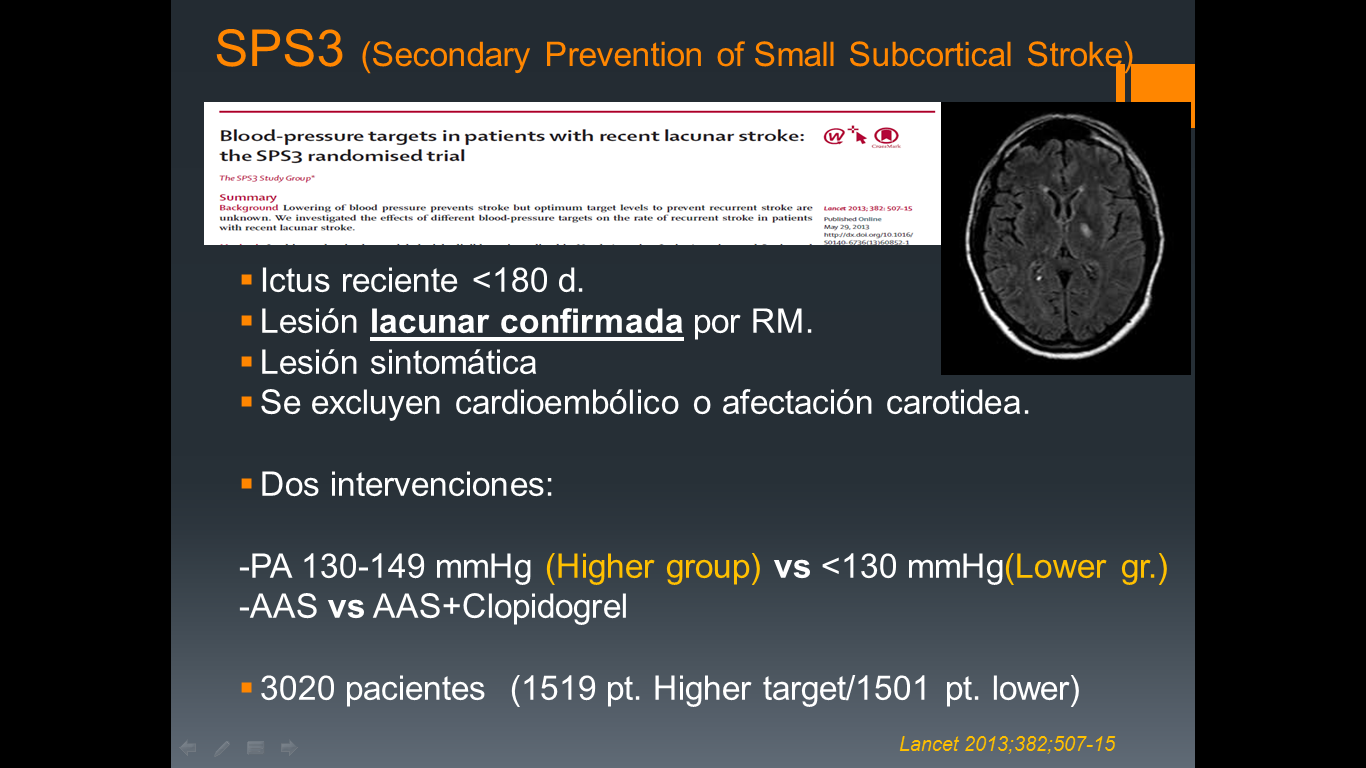
In subacute phase (> 7d) decreased to normal limits depend TA if any vascular occlusion or stenosis where the decrease should be more gradual, even somewhat higher (> 140/90) limits.
Drugs that are ideally use ACE inhibitors, ARBs, calcium antagonist and diuretic indapamide or hidroclorotizada type. Drugs such as alpha blockers (doxazosin) or beta-blockers aren´t of choice but could be used to treat besides another comorbidity as benign prostate hyperplasia in the case of doxazosin or ischemic heart disease in case of beta-blockers.
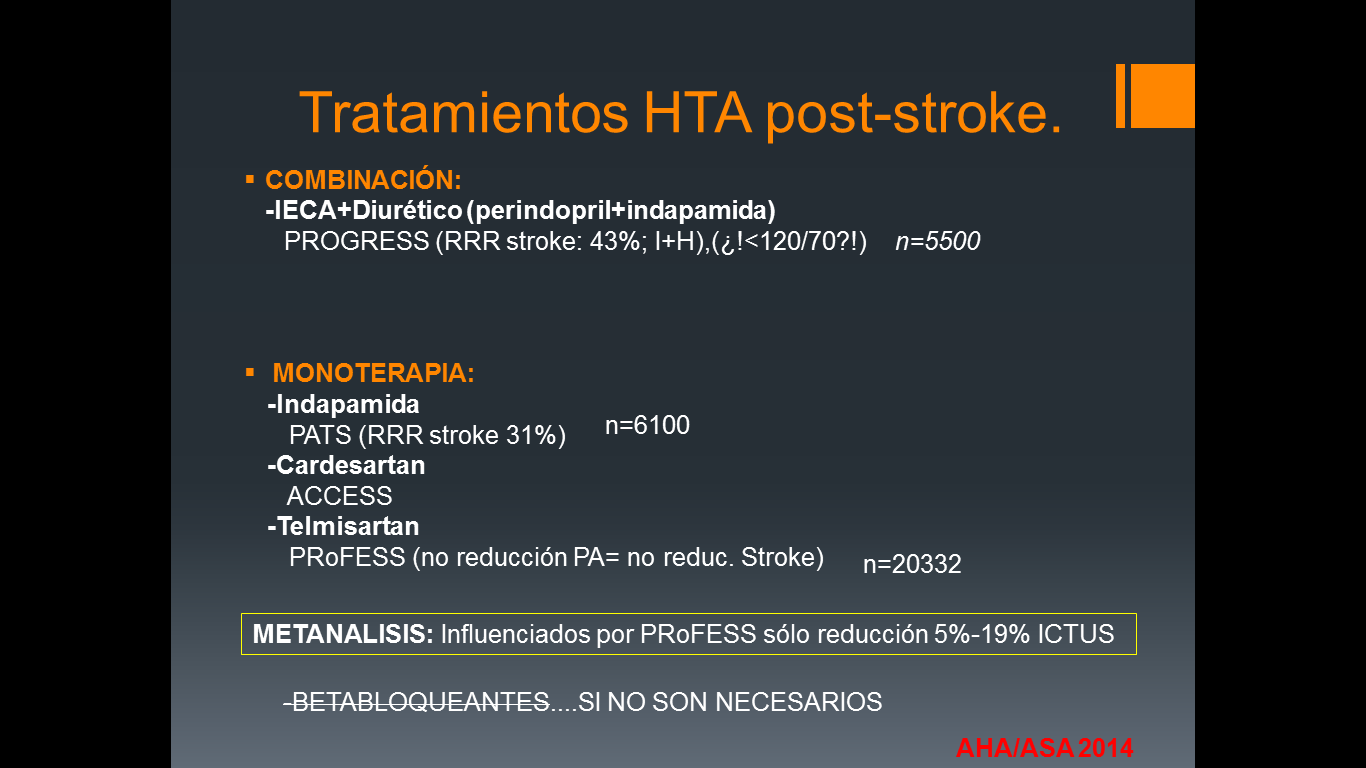
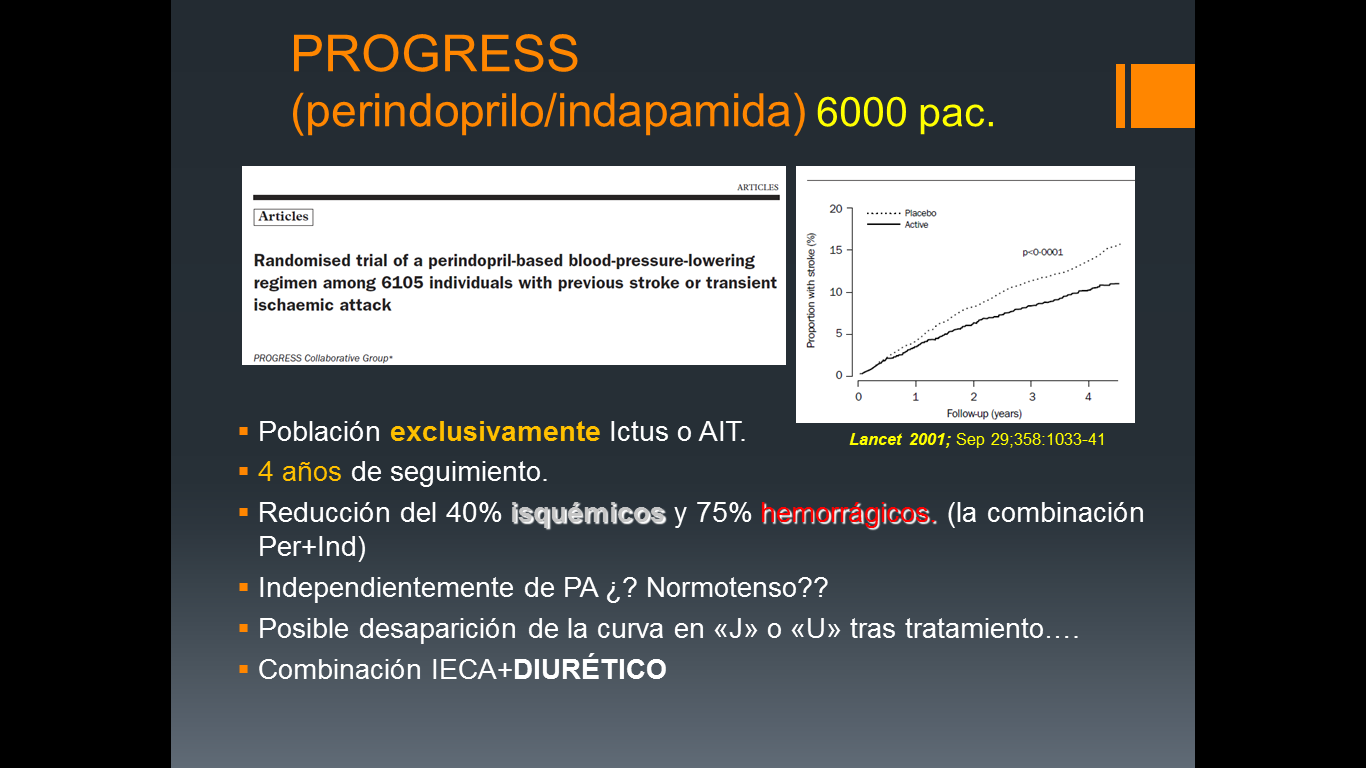
One of the few studies demonstrated hypertensives were usefulness in secondary prevention of stroke was the PROGRESS (perindopril-indapamide) with reduced ischemic events and bleeding after use of the ACE inhibitor and diuretic combination. Even in patients “considered normotensive” benefit was demonstrated with virtually no side effects, however this group were “false normotensive” because if it was considered normotensive low blod pressure 160/100. Few treated normotensive initial figures presented below 130/80, but based on this study was considered and accepted in some groups the idea of dealing with ACE inhibitors including normotensive. Currently this recommendation of treat normotensive should only be assessed if patients with other comorbidities such as heart failure, heart ischemic disease where the use of ACE inhibitors may have some benefit in these diseases.
One of the paradigms and quite common is the fact despise the diuretic as hypotensive when their synergistic effect by the ACE is extremely important. Probably the low fluid intake stroke in these patients by the fear of low output in patients with vascular stenosis makes little is prescribed. As in primary prevention should be monitored renal function, electrolytes after starting any diuretic. In our experience a precaution that should be considered is its use in patients with a history of gout given the frequent occurrence of an attack of gout in a patient at rest and immobilization after stroke. The use of a diuretic may worsen or precipitate it and therefore in patients with this background does not seem useful.
Anyway anxiety, pain, standing and ambulation can cause fluctuations in the level of hypertension despite excellent control and therapeutic management of blood pressure. Water balances and analytical control are very important in this group of patients.