Stroke code allows urgent assessment by a neurologist of patients with a suspected neurological injury as stroke. The stroke center must have a 24h CT to rule out hemorrhagic or other non-ischemic pathology clinic (stroke-mimic). Then neurologist confirmed the diagnosis and treatment as reperfusion options (thrombolysis, thrombectomy).
The assessment of neurological injury can be checked at patient´s home or notify and performed to Emergency Transport Servicie with Cincinatti scale. The presence of any of these symptoms, in patients without major comorbidities (valued at Rankin scale) requires activation code stroke.
Enabling this code call a warning to central SEM and thence to the receiving center that has TAC / 24h and neurology / 24h to establish the diagnosis. Sometimes the patient is at same stroke center and its activation entail intrahospital urgent neurological assessment.
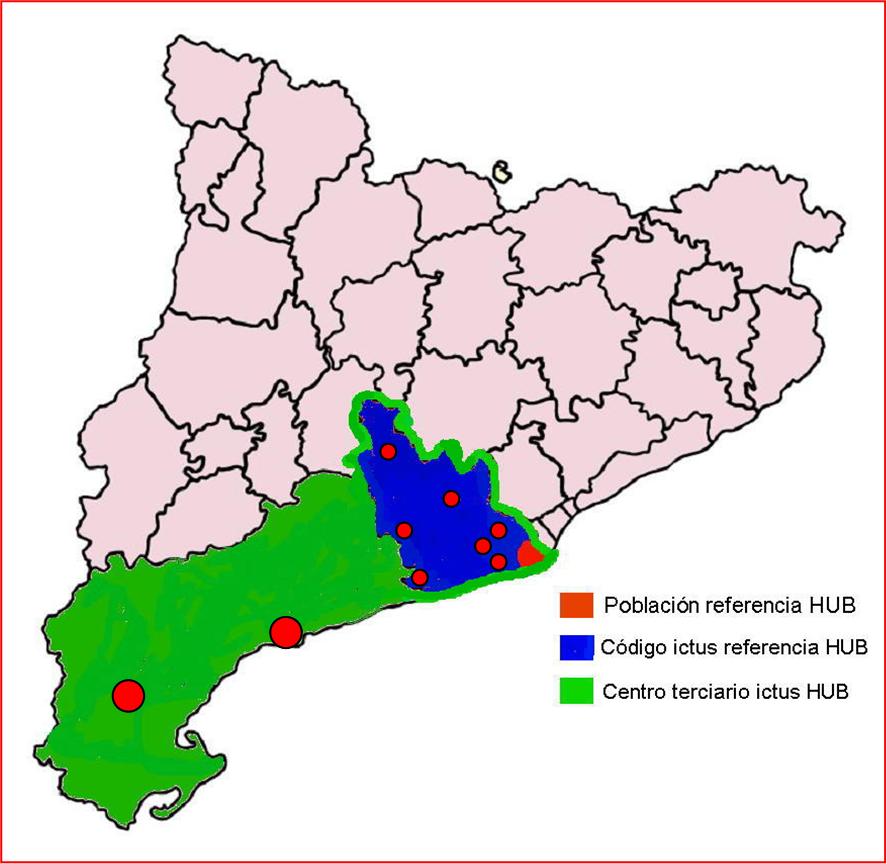
It aims to reduce as far as possible the time to establish the diagnosis because it will allow in case of bleeding control the factors that caused and ischemic strokes can choose ischemic reperfusion therapies. Each geographical area has its stroke code reference centers which in turn can be tertiary center for more complex treatments such as thrombectomy or endovascular treatments or treatment of SHA. In this case the center may be the receiver of the otherprimary centers with stroke codes that do not have this technology.